A clinical case for explaining how much important is to perform simultaneous horizontal binocular VHIT
A 47-year-old woman comes to my office complaining of the appearance of a set of symptoms for a few months.
The most relevant were the following: double vision, blurred vision, oscillopsia, visual delay, difficulty following moving objects, instability with eye or head movements (particularly in horizontal gaze). At the onset she went to an ophthalmologist, but the evaluation carried out did not reveal any pathological elements. Looking at the report I immediately realized that an important element had been omitted: the evaluation of extrinsic ocular motility.
By performing the bedside exam, I began to collect very substantial diagnostic clues. The video-oculographic recording transformed suspicions into certainties. At this point however, as usual, I performed a VHIT and the possibility of analyzing the ocular movements of both eyes provided me with a detailed description of the clinical picture.
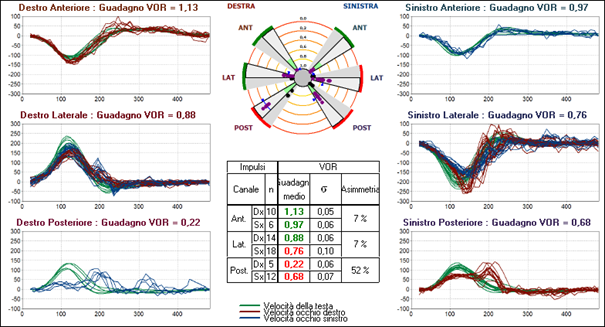
Here is the result of the exam.
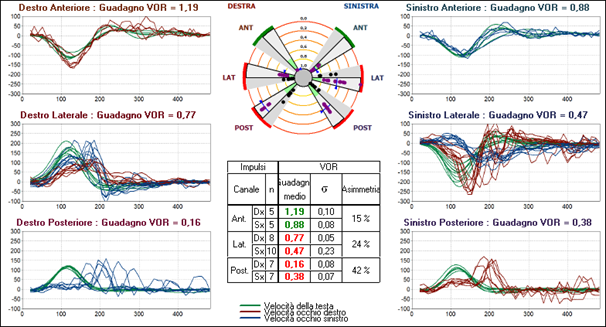
The analysis highlights: (1) the dissociated oculomotor response for impulses executed in the horizontal plane, (2) the reduction in gain for the left lateral and posterior canals and, more evidently, for the right posterior one and (3) the presence of corrective saccades, clearly evident for the two posterior canals.
To get more information I analyze the exam using the gaze position graph and these are the results. The position of the head is in green, the right eye is in red, and the left eye is in blue.
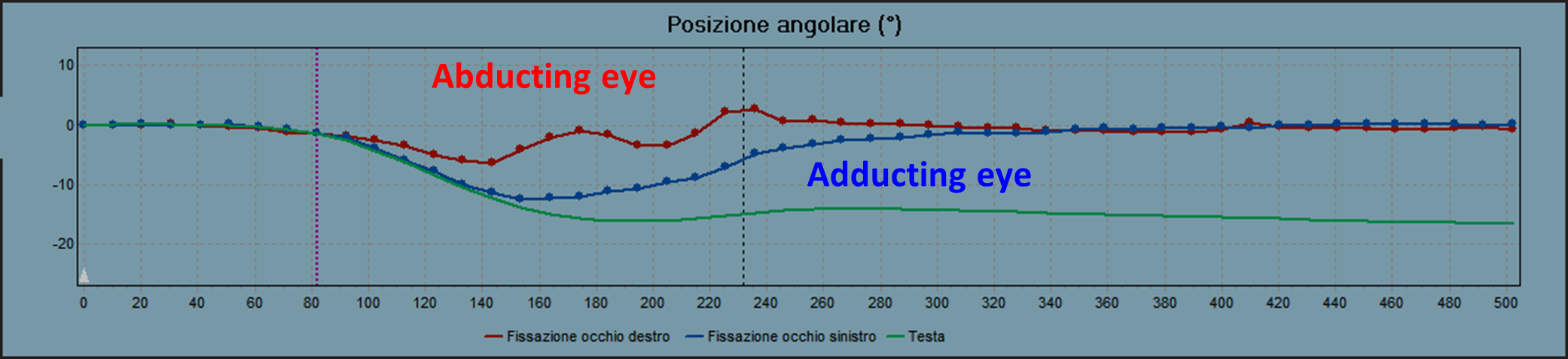
During the movement of the head to the left, the right eye (the abducted eye) misses the target slightly and reaches it with a couple of saccades; the left eye (the adducted eye) consistently misses the target and slowly reaches it with a glissade. The left eye, moving further away from the zero of the gaze position graphs, consequently, expresses a reduced gain.
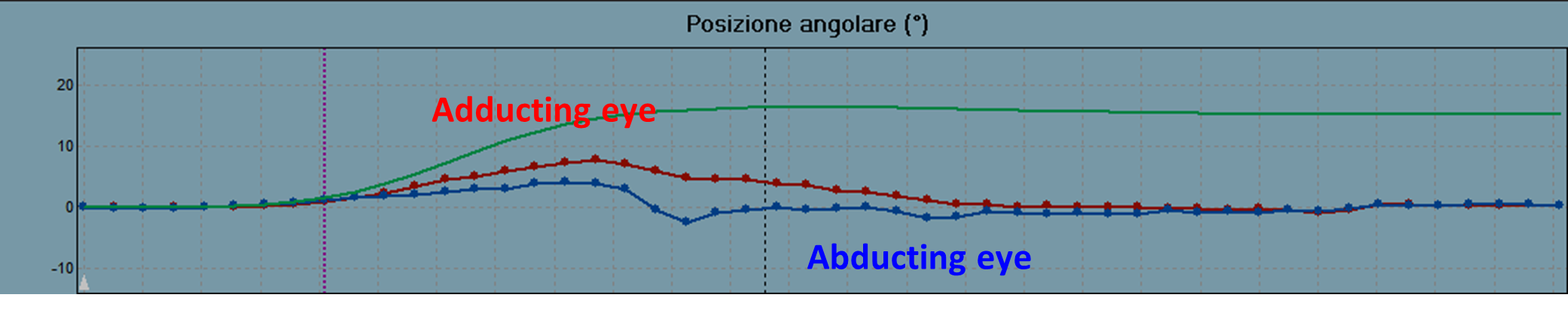
During the movement of the head to the right the opposite occurs. The right eye (adducted eye) reaches the target with a glissade and the left eye (the abducted one) with saccades. In this case, the right eye, moving further away from the zero of the gaze position graphs, consequently, expresses a reduced gain.
The pattern described above is typical of InterNuclear Ohthalmolplegia (INO), as is the reduction in VOR gain starting from the contralateral posterior canal and from the ipsilateral lateral canal.
The diagnosis is that of a bilateral INO, more evident on the left. Neurological evaluation and MRI confirmed MS RR type. The patient began therapy with Tecfidera.
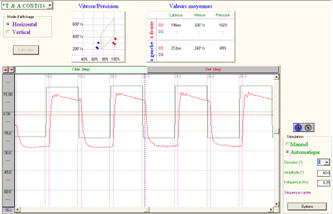
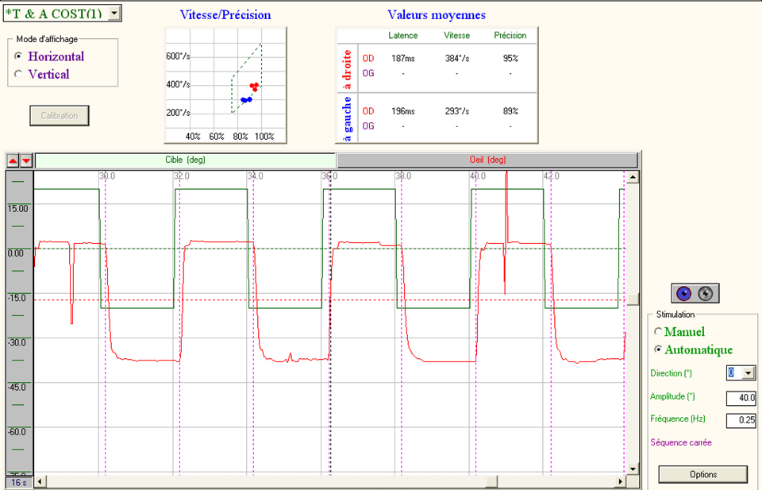
I add a screenshot of the saccadic test in VOG, with camera on the left eye.
One year later, how has the clinical and instrumental picture changed?
There was a clear improvement in the symptoms, with the disappearance of double vision, blurred vision and dizziness with eye or head movements (particularly horizontal gaze). Oscillopsia, visual lag and difficulty in tracking moving objects were reduced in a lesser extent.
At VHIT morphology and gains improved, although the dissociation of eye movements between the right eye and left eye after a horizontal impulse directed to the left persisted. Here is the result of the exam.
The improvement is also evident in the gaze position traces:
- Leftward head movement.

- Rightward head movement.

Saccadic movements normalized.
Being able to compare the movements of both eyes on the horizontal plane is essential to avoid misdiagnosis related to the recording performed on a single eye.

Enrico Armato
Enrico Armato è stato dirigente medico ORL presso ULSS3 Regione Veneto. Ha oltre 35 anni di esperienza come specialista in otorinolaringoiatria, con particolare attenzione alla chirurgia del collo. La sua vera passione è l'otoneurologia. Da molti anni si interessa della valutazione funzionale dei pazienti vertiginosi. È autore del libro “The Video Head Impulse Test - Theoretical and practical aspects” e coautore di numerosi articoli in letteratura nazionale e internazionale. E’ inoltre professore a contratto con L'Università di Padova, Dipartimento di Neuroscienze, corso di Laurea in Tecniche Audiometriche. Enrico collabora con Inventis da diversi anni ed è figura di riferimento per tutto ciò che concerne il mondo vestibolare.

 International - English
International - English Italia - Italiano
Italia - Italiano France - Français
France - Français USA - English
USA - English